Stanford historian explains how frequent yellow fever epidemics in nineteenth-century Louisiana generated cultural and social norms in its fatal wake.
I was intrigued when I came across the Stanford profile of Kathryn Olivarius, PhD, a historian of 19th-century America. Her research primarily explores how epidemic yellow fever disrupted society in the antebellum South, generating cultural and social norms in its fatal wake. To learn more, I spoke with her recently.
As a historian, what got you interested in fellow fever?
“When I embarked on my PhD, I wanted to write about how slavery changed in Louisiana after 1803 with the Louisiana Purchase, as the region shifted from Spanish and French to American rule. But while sitting in Tulane’s archives and perusing letters, diaries, plantation ledgers and ship manifests, what impressed me the most was how much people spoke about disease. And the disease they feared the most was undoubtedly yellow fever — a disease that struck antebellum New Orleans at epidemic levels nearly every third summer.
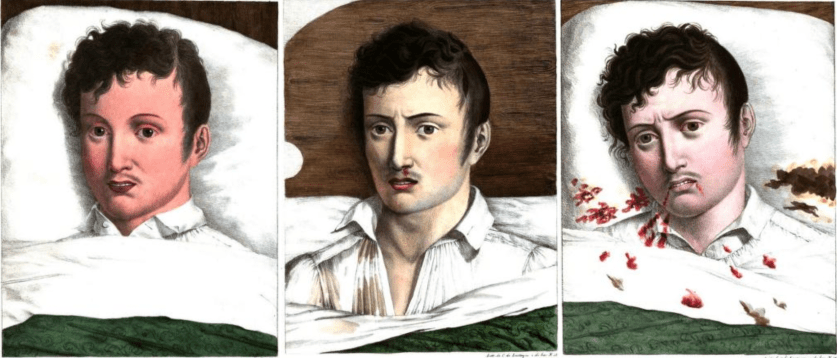
Yellow fever victims experienced a sudden onset of headache, back pains, jaundice, nausea and chills. Within days, they oozed blood through their external orifices, writhed in pain and vomited up partly coagulated blood. About half of all people who contracted yellow fever in the 19th century died, while the survivors gained lifetime immunity.
In my view, yellow fever played a critical role in Louisiana’s asymmetrical social organization, on the schedule and character of the cotton market, on capitalism itself and on the entire system and ideology of racial slavery. So I decided to focus on the disease for my PhD and my forthcoming book.”
How did the disease impact the social structure of 19th-century Louisiana?
“Antebellum New Orleans sat at the heart of America’s slave and cotton kingdoms. But it was also the nation’s necropolis, the city of the dead, with yellow fever routinely killing about 8 percent of its population between July and October. In some neighborhoods — particularly those with high densities of immunologically-naive recent immigrants from Germany, Ireland and the American North — yellow fever deaths could reach 20 or even 30 percent.
These repeated epidemics generated a hierarchy of ‘acclimated’ survivors who leveraged their immunity for social, economic and political power and ‘unacclimated’ recent immigrants who languished in social and professional purgatory. Until whites could prove they were acclimated, they struggled to find steady, well-paid employment, housing, spouses and a political voice. From the employer’s perspective, it wasted time and money to train someone for a detail-oriented job only to watch him sicken and die by the autumn.”
How did this affect slavery?
“Because of the disease, the commercial-civic elite of New Orleans argued that they required large-scale black slavery — publicly proclaiming that black people were naturally immune to the disease based on spurious and racially-specific visions of medicine and biology. It became a powerful proslavery argument with many whites claiming that black slavery was natural, even humanitarian, as it distanced white people from labor, spaces and activities that would kill them. Some even argued black immunity signaled divine sanction for widespread slavery, with God creating black slaves specifically to labor in the cane and sugar fields of the Mississippi Valley.
But in private, most slavers would not buy an unacclimated slave. The slave market essentially shut down in August, September and October in order to protect the health of potential buyers and their valuable slave property. This inconsistency suggests that the widespread belief in black immunity was less a reflection of biological reality but instead a social tool, a means to epidemiologically-justify racial slavery.”
Do you believe anything similar is happening today?
“Yellow fever still kills thousands of people each year. It’s endemic in 47 countries, mostly in Africa and Central and South America. The Intergovernmental Panel on Climate Change’s report released last year also suggests that Americans may become more familiar with this disease again as ecologies change and mosquito populations migrate. Zika, spread by the same mosquito as yellow fever, has been an increasing problem in recent years.
In terms of the social impact of disease, there are certainly modern analogues of societies in the midst of terrifying epidemics rationalizing mass death or singling out certain marginalized groups as the cause. The most obvious comparison in the U.S. is probably HIV/AIDS in the 1980s with gay people, intravenous drug users and Haitians who were blamed for the disease’s spread and who faced severe discrimination on the basis of their alleged-vulnerability.”
This is a reposting of my Scope blog story, courtesy of Stanford School of Medicine.






{kind=link}
{kind=link}