Mike Garland (BA ’72) donates to Berkeley Physics to give back to the university that helped change his life. In addition to supporting the Michael M. Garland Chair in Physics since 2008, he and his wife, Gigi Coe, recently founded the Shining Lights Program—providing leadership training to women-identifying graduate students and postdoctoral scholars in Berkeley’s mathematical and physical sciences.
“I’ve always felt women are equally capable, if not more so, than men. But there aren’t enough of them in leadership positions, especially in the physical sciences,” Garland says. “We wanted to elevate women to become more successful leaders by providing diverse leadership coaching and networking.”
Garland and Coe initiated and funded the program, with the enthusiastic support of Dean of Mathematical and Physical Sciences Steve Kahn and Assistant Dean of Development Maria Hjelm. However, Shining Lights was run by Berkeley Physics Associate Professor Gabriel Orebi Gann.
“All the credit goes to Gabriel. She grabbed the idea and ran with it. And she understands better than us what content these women need, including critical soft skills like working with an actor to learn a power stance,” says Garland.
The success of the program was clear at the graduation this spring. One thrilled graduate’s mother flew out for the ceremony. Former Chancellor Carol Christ came back to give an inspiring speech. And several graduates spoke about how the program had already made a difference in their lives.
“I was amazed at the level of camaraderie and enthusiasm at the graduation. They really lit up about the relationships they’ve developed with each other,” says Garland. “The joyful, formal celebration really showed that Berkeley was the right place for Shining Lights.”
“As far as we are concerned, the first year of Shining Lights was an enormous success. We hope to see it build and grow, maybe into other areas in science,” adds Coe. “And we may need to add additional training for young scientists to navigate these turbulent times.”
Scientists across the nation are both fascinated by the work done at the Department of Energy’s national laboratories and could make important contributions to that work. Still, many of them – especially those at institutions historically underrepresented in the research community – don’t have the financial support or pathways they’d need to take part.
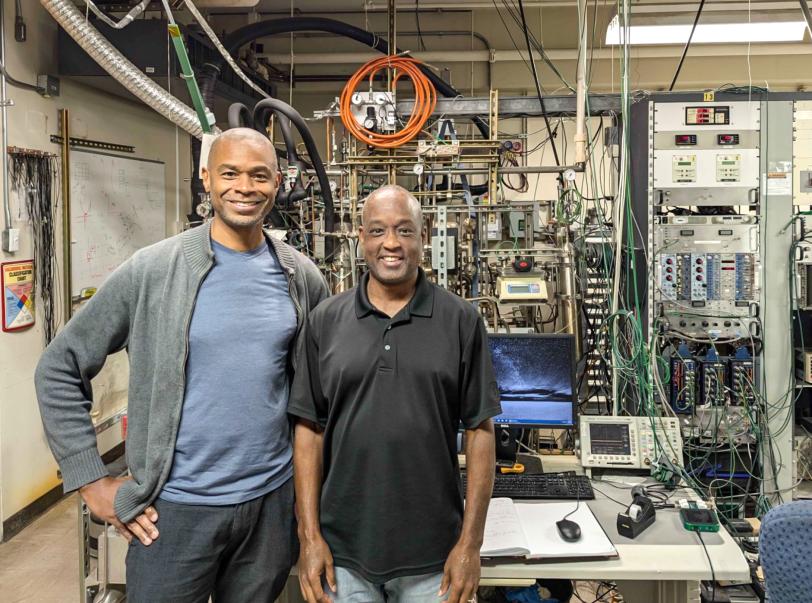
Such was the case for Southern University and A&M College’s Fred Lacy and Skyline College’s Kolo Wamba – but this summer both got a chance to learn from and contribute to research at DOE’s SLAC National Accelerator Laboratory through DOE’s Visiting Faculty Program (VFP).
The program aims to enhance the faculty’s research competitiveness and STEM instruction, while helping to expand and diversify the workforce vital to DOE’s mission areas. VFP is designed for full-time faculty from schools that are not major research universities, known as R1 universities, or from historically black colleges or universities, said Hillary Freeman, SLAC’s STEM Education Program Manager. “Selected faculty members participate in research that they are interested in alongside SLAC scientists with similar interests,” Freeman said. “The goals include providing these faculty with access to world class research, learning new skills that can be brought back to the classroom to help develop the next generation of scientists, and perhaps moving their home institution towards an R1 status.”
Freeman noted that faculty can also bring students with them, which helps further the program’s goals.
“We need to create more awareness about the Visiting Faculty Program, which among other things gives our researchers the opportunity to leverage relationships with minority-serving institutions and the faculty who work there,” said Natalie Holder, chief diversity officer at SLAC. “It’s incredibly important that our researchers meet these visiting faculty, work alongside them, and exchange information.”
Enhancing microelectronic devices
Lacy, a professor and the chair of the electrical engineering department at Southern University and A&M College in Baton Rouge, Louisiana, participated in the program to grow as a research engineer and person, as well as share the experience with Southern University’s students in the classroom.
Having no previous affiliation with DOE laboratories, Lacy established the partnership with SLAC through the VFP application process and ended up connecting with SLAC scientist Sander Breur in the Instrumentation Division of SLAC’s Technology Innovation Directorate (TID). “The Instrumentation Division consists of about 60 engineers, technicians, and scientists who fully focus on creating the technical capabilities that many of SLAC’s experiments require,” Breur said. “To conduct the required research, and help train the next generation of instrumentation experts, TID actively works on creating connections such as with the Visiting Faculty Program.”
This summer, Lacy tackled two projects to help develop microelectronic devices that may be included in future detector designs. The first, Tiny Machine Learning (TinyML), is led by SLAC engineers Dionisio Doering and Abhilasha Dave. The effort incorporates machine learning algorithms in microelectronic circuits to provide “edge computing,” enabling data to be analyzed closer to sensors and in real time instead of processing data remotely after collection. The main challenge of edge computing is having enough memory and hardware to perform and store the calculations.
“Researchers typically perform calculations by running really large, complex computer programs on large computers. If you reduce the number of lines of code and the digits representing each number in the calculations, then you can reduce the amount of necessary hardware,” said Lacy. “But how does that affect accuracy? What trade-offs are acceptable for particular applications? That’s what we’re exploring.”
In addition to the potential application of providing local, real-time data analysis for physics experiments, TinyML could be used in implanted or wearable devices for healthcare monitoring or in automotive systems for detecting drowsy drivers.
Lacy also worked towards developing application-specific integrated circuits that perform better in harsh environments for cryogenic and radiation experiments. This hardware-based Power Management through Integrated Capacitors (PMIC) project is led by SLAC engineers Hugo Hernandez, Aldo Perez, and Lorenzo Rota.
Currently these integrated circuits (or computer chips) need external capacitors to provide and store electric charge, but these capacitors are bulky and tend to be too contaminated by trace radiative impurities for some experiments. To address that issue, the PMIC project is exploring microfabrication techniques to integrate capacitors into the computer chips themselves. This summer, Lacy did preliminary materials testing of small capacitors in super cold environments.
“Working with both SLAC groups was a fabulous experience,” said Lacy. “I plan to continue the TinyML project at my home institution and will start involving students. I also plan to teach them the basics of the PMIC project, so they can immediately make an impact when I bring them to SLAC, hopefully next summer. But I’ll also mention my VFP experience to students in all of my classes to open their minds to different career options, because the national labs aren’t on their radar the way Fortune 500 companies are.”
Improving xenon purity monitoring
Wamba, a physics and astronomy professor at Skyline College in San Bruno, California, has a longstanding relationship with SLAC – including earning a PhD in applied physics at Stanford University based on performing research for the EXO-200 experiment, the predecessor of nEXO, with Martin Breidenbach, a professor emeritus at SLAC.
The nEXO project is a proposed international nuclear physics experiment that will use an enormous tank of liquid xenon to search for neutrinoless double beta decay. If this rare and hypothetical process is discovered, it would prove that neutrinos are their own antiparticles and help physicists understand various mysteries of the universe, including why there is more matter than antimatter in the universe.
Wamba formally joined the nEXO collaboration as a faculty member in 2021, and has previously brought students to SLAC through the DOE’s Research Traineeships to Broaden and Diversify pilot program. Rather than continuing this work through Skyline College’s new RENEW program, Wamba applied to VFP.
“The VFP is a good fit for supporting my nEXO research because the funding program is limited to summer, so it doesn’t conflict with my teaching responsibilities,” Wamba said.
This summer, Wamba worked with SLAC physicist Peter Rowson on nEXO’s xenon purity monitor (XPM) system, a custom-built apparatus used to determine the chemical purity of a liquid xenon sample after it has been exposed to materials that could generate impurities. Originally, Wamba planned to run the XPM a “bunch of times,” acquiring and analyzing various data sets under different conditions.
Although troubles with a faulty power supply got in the way of those plans, there was a silver lining. “We didn’t get to run the xenon purity monitor as many times as I was hoping this summer,” Wamba explained. “But on the flip side, this gave me an unexpected opportunity to construct hardware that simulates the XPM so we can characterize its systematic errors. I wasn’t even thinking of doing that at the beginning.”
Wamba programed a waveform generator to create a “ground truth” signal that would mimic the output of the XPM. This hardware simulator was then used in place of the XPM, running the signal through the entire system and analysis chain. By comparing the resulting signal with the ground truth one, the systematic errors were characterized, using fewer assumptions than a previously planned software simulator.
Wamba plans to reapply to the Visiting Faculty Program and bring at least one student next summer to do other nEXO research projects. “I plan to use project-based learning where I guide students and teach them whatever they need as it comes up.”
Holder was happy to hear that Lacy and Wamba both intend to bring students to SLAC. “The goal for the future is to have the visiting faculty bring some of their students along with them, and to ignite that interest in their students to come back eventually to study, maybe at Stanford while pursuing their PhDs, and then eventually to become our colleagues as staff, researchers, faculty, and maybe even one day as a lab director,” Holder said.
Lacy and Wamba were supported by the DOE’s Visiting Faculty Program, a component of DOE’s Workforce Development for Teachers and Scientists program. SLAC researchers were supported in part by the DOE Office of Science.
Every living organism on Earth has a genome, the complete set of DNA containing all of the information needed to develop and maintain the organism. Humans inherit three billion long strings of DNA called chromosomes from each parent, so your genome can help identify your personal ancestry. But genomes can also identify the movement of human populations based on who is similar to whom.
Carlos Bustamante, PhD, a professor of biomedical data science, of genetics and of biology at Stanford, discusses the blossoming uses of genomes on a recent episode of “The Future of Everything” radio show.
For example, Bustamante told host Russ Altman, MD, PhD, a professor of bioengineering, of genetics, of medicine and of biomedical data science, about the genomic fingerprints of the history of slavery in the United States. As part of an international collaboration, he studied the DNA of modern individuals and individuals from slave cemeteries, tracing their history to particular tribal groups in Africa.
“A lot of that history has been lost and African Americans want to reclaim parts of that history using DNA,” Bustamante said. “What’s interesting, at least in the United States, is that most of the slave ships went first to the Caribbean and Brazil. Only a couple hundred thousand people came in straight to the Port of Charleston. So the history of the slave trade is actually written in the DNA of the Caribbean, Brazilian and U.S. African descendant populations.”
But that is only one of the many genomic applications discussed on the episode. Another important use is predicting disease risks. Genetic tests are now available for many hereditary conditions, including cancer risk assessment, at Stanford.
This raises a challenge, however, because our knowledge of DNA is primarily based on people of European descent. As Bustamante explained, this occurred because European countries were the first to recognize the potential impact that DNA sequencing could have on health care, once the cost of DNA sequencing technology plummeted.
“They invested quickly and by the year, say 2009, they’d done about a thousand studies and 95 percent of the participants in those studies were of European descent — be they from the countries in Europe or in Iceland.”
Since humans are 99.9 percent identical in their genetic makeup, maybe this doesn’t sound like a problem. But Bustamante said the differences may be important because they could help lead to improvements in health care. He described this lack of diversity as both a problem and an opportunity.
Take blond hair, for example. Bustamante explained that two main populations have blond hair: Europeans and Melanesians from the Solomon Islands. When the scientists started a research project, they hypothesized that a European went to Melanesia and had a lot of kids. But that isn’t what the genetics showed.
“The genetics of blond hair in Europe are different than the genetics of blond hair in Melanesia. They look the same, but it turns out that the underlying genes are different,” he said. “And why is that interesting? From the point of view of medical genetics, if this is true for blond hair — which is about as simple a trait as you can get — what about diabetes? Why would we assume the genetic basis of diabetes is the same in every population, when we know diabetes actually presents differently in different populations?”
He also argued that new drug discovery would be more successful if it was based on genetic leads. Cholesterol lowering drugs called PCSK9 inhibitors, for instance, were found by studying families with naturally high or low levels of cholesterol. Successes like these are the reason he thinks it’s important to study diverse populations.
“If we spread our bets across different human populations, we’re much more likely to find interesting biology that then benefits everybody,” he said. “Because these cholesterol lowering drugs aren’t just good for those people with high cholesterol for genetic reasons. That’s the key. You can mimic it in others and it benefits everybody.”
Of course, the potential for genomics goes beyond human applications. Altman and Bustamante also discuss plant and animal uses, including designing your dream dog.
This is a reposting of my Scope blog story, courtesy of Stanford School of Medicine.
Photo, of Rania Awaad giving a recent talk, by Anum Ahmad
Prior to studying medicine, Stanford psychiatrist Rania Awaad, MD, studied Islamic law. As a local religious leader, she said that many people in her community are actually surprised to learn that she’s also a physician.
However, this dual training is at the heart of Awaad’s research and clinical work, which focuses on the mental health needs of Muslims. I recently spoke with her to learn more.
What are the mental health challenges faced by Muslims?
“In our recent sociopolitical climate, there’s been quite a bit of negative focus on Muslims and other groups. And we have the highest level of hate crimes against Muslims ever in American history — about six times higher than post 9/11.
In the Bay Area, we have a consortium of mental health and general medical providers who are trying to figure out how Islamophobia — the fear of the Islam religion or Muslims — affects the general health of Muslims. So far, we’ve seen a lot of anxiety, depression and post-traumatic stress disorder.
There’s already quite a bit of PTSD within the community, because many Muslims that immigrate to America come from areas of conflict. Current policies can trigger immigrants’ underlying PTSD, anxiety and depression, as I recently described in the American Journal of Psychiatry.”
Are there barriers to mental health care for your patients?
“There’s a lot of paranoia about medical providers documenting their issues in an electronic medical record. They’re afraid this medical information will be combined with a Muslim registry. Initially we told patients not to worry, because unconstitutional things like that don’t happen here. But then the travel ban helped substantiated their fears.
There are also barriers directly tied to faith beliefs — concepts like the evil eye or spirits. If someone is having psychosis, for example, people may say he is possessed and should be taken to his religious leader instead of a mental health professional.”
What can you do to overcome these challenges?
“Mental health professionals can approach a patient’s faith leader for a religious consultation. I help train chaplains and imams and I’m also teaching doctors to engage with faith leaders. For many people, their faith is a source of strength and support. So leaving that out completely means that you’re not really providing adequate, holistic care.
There are a limited number of mental health professionals proficient in understanding the Muslim faith and culture. Through the Khalil Center, I’m working with other dual-trained practitioners to develop a manual, book and training seminar on Islamic psychology from a practical clinical perspective. We’re trying to provide guidance for practitioners without Islamic training to work with this unique minority group.”
How did you end up specializing in the mental health needs of Muslims?
“I thought I was going to be an ob/gyn. But during medical school, I married my husband who is an imam and a director of a nonprofit. At one point he told me what our community really needs is someone who can work in mental health, based on what he saw as a community leader. He inspired me to become a psychiatrist.
I also feel my dual training was meant to be. In high school I embarked on a lifelong journey of formal Islamic studies training. I’m currently a professor of Islamic Law at Zaytuna College, a Muslim liberal arts college in Berkeley. My dual training kickstarted the Stanford Muslim Mental Health Lab and Wellness Program that I founded and direct, and it has allowed me to lay the groundwork to train others.”
What are some other things you’re working on?
“The SMMH Lab is part of a consortium that is studying the effectiveness of integrating faith concepts with therapy for different faith communities — Muslim, Jewish and Christian groups. We’re using evidence-based, objective metrics like the depression inventory scale.
I also oversee the Bay Area Muslim Mental Health Professionals group, which has led to many other initiatives like a Bay Area Muslim mental health community advisory board and a crisis response team.”
This is a reposting of my Scope blog story, courtesy of Stanford School of Medicine.