The hit new crime thriller Blindspotis about a mysterious woman, Jane Doe, who is covered in extensive full-body tattoos. If Jane Doe were a real woman who ever needed medical imaging, she might need to be concerned.
In a case report published recently in the journal Obstetrics & Gynecology, researchers found that extensive tattoos can mimic metastases on images from positron emission tomography (PET) fused with computed tomography (CT). PET-CT imaging is commonly used to detect cancer, determine whether the cancer has spread and guide treatment decisions. A false-positive finding can result in unnecessary or incorrect treatment.
Ramez N. Eskander, MD, assistant professor of obstetrics and gynecology at UC Irvine, and his colleagues describe the case study of a 32-year-old woman with cervical cancer and extensive tattoos. The pre-operative PET-CT scan using fluorine-18-deoxyglucose confirmed that there was a large cervical cancer mass, but the scan also identified two ileac lymph nodes as suspicious for metastatic disease. However, final pathology showed extensive deposition of tattoo ink and no malignant cells in those ileac lymph nodes.
It is believed that carbon particles in the tattoo pigment migrate to the nearby lymph nodes through macrophages, using mechanisms similar to those seen in malignant melanoma. The researchers explain in their case report:
Our literature search yielded case reports describing the migration of tattoo ink to regional lymph nodes in patients with breast cancer, melanoma, testicular seminoma, and vulvar squamous cell carcinoma, making it difficult to differentiate grossly between the pigment and the metastatic disease, resulting in unnecessary treatment.
The authors warn other physicians to be aware of the possible effects of tattoo ink on PET-CT findings when formulating treatment plans, particularly for patients with extensive tattoos.
This is a reposting of my Scope blog story, courtesy of Stanford School of Medicine.
A recentNew York Timesblog entryeditorialized on the worldwide shortage of transplant kidneys, raising the question of whether it’s time to compensate kidney donors to meet the growing need. The blog echoed the debate that is emerging in the United States among some doctors, medical societies, and groups that oversee organ transplants.
Taboos against paying for transplant organs are powerful. But these may be overcome by necessity, since the demand for transplant kidneys is growing at an alarming rate largely due to kidney failure from diabetes, high blood pressure and obesity-related diseases.According tothe National Kidney Foundation, 450,000 Americans are on dialysis and the severe shortage of transplant kidneys in the U.S. results in 12 patient deaths each day.
Laying the groundwork for change, a collaboration of nephrology and finance experts, including Philip J. Held, PhD, a Stanford consulting professor of nephrology, performed a comprehensive cost-benefit analysis of a proposed government program for kidney donor compensation. In astudypublished last week in the American Journal of Transplantation, the authors estimate the shortage of transplant kidneys would be eliminated within five years if the government compensates living kidney donors $45,000 and the estates of deceased donors $10,000. The proposed compensation would also include an insurance policy against any health problems that might result from the donation.
The authors’ analysis shows that the benefits of a donor compensation program would greatly exceed the costs for society in general and taxpayers in particular. The researchers calculate the monetary value of a longer and healthier life for each kidney recipient at $1.3 million, with the added bonus of saving $1.5 million for not needing expensive dialysis treatments. After subtracting from these benefits the cost of transplants, society would enjoy a net welfare gain of $1.9 million over the lifetime of each kidney recipient. Since taxpayers currently pay about 75 percent of the cost of both dialysis and kidney transplants, this represents a taxpayer savings of about $400,000 per kidney recipient.
One of the main arguments against kidney donor compensation is that rich people would buy kidneys from poor people, exploiting them and causing them harm. The authors argue that the opposite is true because the poor, especially poor African Americans, are overrepresented on the kidney waiting list – so they would enjoy the greatest benefit.
The researchers summarized their findings in a press release supplied to our office:
“In sum, having the government compensate kidney donors would be a win-win-win situation. Kidney recipients would enjoy much longer and healthier lives. Kidney donors would receive compensation for their gift of life, whereas now they receive nothing. And taxpayers would save money because transplantation is not only a more effective treatment for kidney failure than dialysis, it is a much less expensive one.”
This is a repost of my Scope blog story, courtesy of Stanford School of Medicine.
The device on the golden fingertip is the skin-like sensor developed by Stanford engineers. (Bao Lab)
A hand without a sense of touch doesn’t really feel like a hand, many amputees describe. It’s more like a pliers that can be manipulated by sending signals from the brain to the prosthetic device. They dream of being able to delicately pick up a glass or to feel the touch of a loved one’s hand.
Stanford chemical engineering professor Zhenan Bao, PhD, and her team have spent a decade trying to help make this dream a reality, by developing a material that mimics skin and its sensory functions. Taking a big step towards this goal, they have now created a skin-like material that can tell the difference between a soft touch and a firm handshake.
Their artificial skin has two layers. The bottom layer acts as a circuit that transports pulses of electricity to nerve cells and translates these signals into biochemical stimuli that the nerve cells can detect. The top layer is a sensing mechanism composed of thin plastic embedded with billions of carbon nanotubes. When pressure is put on the plastic, the nanotubes are squeezed closer together enabling them to conduct electricity. What’s new is that the top layer can now detect pressure over the same range as human skin.
This allowed the plastic sensor to mimic human skin, which transmits pressure information to the brain as short pulses of electricity, similar to Morse code. Increasing pressure on the waffled nanotubes squeezes them even closer together, allowing more electricity to flow through the sensor, and those varied impulses are sent as short pulses to the sensing mechanism. Remove pressure, and the flow of pulses relaxes, indicating light touch. Remove all pressure and the pulses cease entirely.
A paper describing Bao’s new research has just been published in Science. As Bao comments in the release, “We have a lot of work to take this from experimental to practical applications. But after spending many years in this work, I now see a clear path where we can take our artificial skin.”
This is a repost of my Scope blog story, courtesy of Stanford School of Medicine.
Morphine is a common narcotic pain reliever with significant side effects (sfxeric/Flickr).
Morphine is a powerful narcotic, commonly used to treat moderate to severe pain from surgery, injury and chronic health conditions like cancer or osteoarthritis. However, morphine has many negative side effects. It can cause drowsiness, nausea, vomiting, dizziness and constipation. More troubling, people can become dependent on it.
According to the Centers for Disease Control and Prevention, narcotic dependence and overdose deaths are a growing health problem in the United States. Narcotic sales quadrupled from 1999 to 2010 and narcotic-related deaths more than tripled from 1999 to 2012. More than 2 million people in the U.S. currently abuse narcotics.
In order to address this problem, researchers have long searched for alternative drugs that effectively relieve pain without inducing dependence as morphine does. A team of researchers now believe they’ve found a good candidate for such a drug, although it will be a long time before this drug, if it proves to be effective, is available in stores.
The LCLS creates the brightest X-ray source on the planet, which researchers need to accurately study the structure of tiny, nanoscale drug compounds.
How Narcotics Work
Narcotics are also called opioid pain relievers, because they block the sensation of pain by binding to opioid receptors within the pain pathway of the brain. A drug can provide pain relief by binding to one of three types of opioid receptors in the brain: delta, mu and kappa. Narcotics like morphine target the opioid mu receptors.
The problem is that long-term use of morphine reduces the number of available opioid mu receptors. As a result, tolerance develops so a higher dose of the drug is needed to achieve the same level of pain relief. Ultimately, prolonged use leads to physical dependence — which is when the neurons adapt to the presence of the drug and function normally only when it’s in the body.
Previous research has shown that administering morphine with another drug that simultaneously blocks the opioid delta receptors prevents this morphine-induced tolerance and dependence. Researchers just need to find the right drug combination with minimal side effects.
Recently, a team of researchers, led by University of Southern California chemistry professor Vadim Cherezov, developed a drug that activates opioid mu receptors while blocking opioid delta receptors. Their drug is derived from a specialized peptide – a naturally occurring chain of amino acids. Their research results were reported in the February issue of Nature Structural and Molecular Biology.
Studying Tiny Crystals
Unfortunately, it is very difficult to study new opioid compounds like the one Cherezov recently developed.
In order to understand the structure of new compounds, scientists usually grow crystals of the compound and then hit them with X-rays. By measuring the angles and intensity of how the X-rays bounce off the crystals, they can produce a three-dimensional picture of the crystal structure.
However, it can be difficult to grow crystals large enough to use this standard method, called X-ray crystallography. Plus, you typically need to freeze the crystal to make it more rigid, rather than study it in natural conditions and temperatures. On top of that, a conventional X-ray beam might blast and destroy the small crystal before you can collect enough data.
Instead, Cherezov’s team used the Linac Coherent Light Source to perform their experiment on tiny crystals at room temperature. LCLS X-ray pulses last just a quadrillionth of a second, or 100 times faster than it takes light to travel the width of a human hair. Yet they are a billion times brighter than a conventional X-ray source.
Using this unique X-ray source with higher-intensity, very short pulses, Cherezov was able to use smaller crystals and still collect terabytes of structural data before the crystals vaporized.
Each crystal the research team prepared was a millionth of a meter and contained many copies of their new opioid compound bound to an opioid receptor. The team placed the crystals in a toothpaste-like gel to simulate the receptors’ natural environment, and then injected a thin stream of this gel into the path of the LCLS X-ray beam.
The resulting structural model was precise enough to show how the new drug molecules bind with the receptor. This atomic-scale map should help scientists develop pain-relieving drugs with fewer negative side effects. It’s likely to to take years, though, before it can be tested in humans.
“This work will provide a solid basis for the design of a new generation of pain relievers with reduced dependency,” Cherezov said in a press release.
Cherezov’s experiment is just one of many performed at the Linac Coherent Light Source.
The LCLS is a Department of Energy User Facility where approximately 600 scientists conduct groundbreaking experiments each year, across many fields, including chemistry, biology, material science, technology and energy science.
Device used by UC Davis researchers to rapidly concentrate stem cells, which are harvested from surgical irrigation fluid during an orthopedic procedure (Courtesy of SynGen Inc).
About 6 million people in North America suffer bone fractures each year and 5 to 10 percent of these patients are resistant to healing, according to the American Academy of Orthopaedic Surgeons. This means that about half a million Americans annually have fractures that don’t heal. UC Davis researchers are developing an improved surgical therapy for such fractures, using stem cells and innovative technology.
After a broken bone is treated, new bone tissue usually begins to form and connect the broken pieces. However, some bone fractures don’t heal due to a lack of adequate stability, blood flow, or large bone loss. For instance, severe bone fractures that are caused by a high-energy car wreck are more likely not to heal. Several other factors increase the risk of non-healing bones, including older age, diabetes, poor nutrition, use of tobacco, and severe anemia. Traditional treatments to address this problem, such as bone grafts taken from another part of the body, often lead to pain, dysfunctional limbs, and disabilities.
In the last several years, the application of stem cells directly to the wound site has emerged as an improved way to treat non-healing fractures. However, acquiring the necessary stem cells from the patient, a matched donor, or embryo is problematic. Ideally the stem cells come directly from the patient, but this requires a painful surgical procedure with general anesthesia during which a large needle is used to retrieve the stem cells from the hip. In addition, the retrieved stem cells need to be isolated before they can be transplanted back into a patient, so a second surgery is required with a long combined recovery period.
“People come to me after suffering for six months or more with a non-healing bone fracture, often after multiple surgeries, infections and hospitalizations,” said Mark Lee, UC Davis associate professor of orthopaedic surgery, in a press release. “Stem cell therapy for these patients can be miraculous, and it is exciting to explore an important new way to improve on its delivery.”
Mark Lee, UC Davis associate professor of orthopedic surgery (Courtesy of UC Davis).
In their new clinical trial, Lee’s team is testing a new SynGen Inc. device that processes the irrigation fluid obtained during an orthopedic procedure. This irrigation fluid contains abundant mesenchymal stem cells and other factors that can be used to help make new blood vessels and improve wound healing.
During the surgery, the irrigation fluid is aspirated and captured. The fluid is then centrifuged and processed using the new SynGen device, which rapidly isolates a concentration of mesenchymal stem cells in less then 30 minutes. These concentrated stem cells are then delivered to the patient’s fracture during the same surgery. The device is about the size of a food processor, so it can be easily used in an operating room.
“The device’s small size and rapid capabilities allow autologous stem cell transplantation to take place during a single operation in the operating room rather than requiring two procedures over a period of weeks,” said Lee in the press release. “This is a dramatic difference that promises to make a real impact on wound healing and patient recovery.”
The UC Davis researchers are already testing this new surgical treatment on patients. However, it is unclear when this treatment could move into general clinical practice.
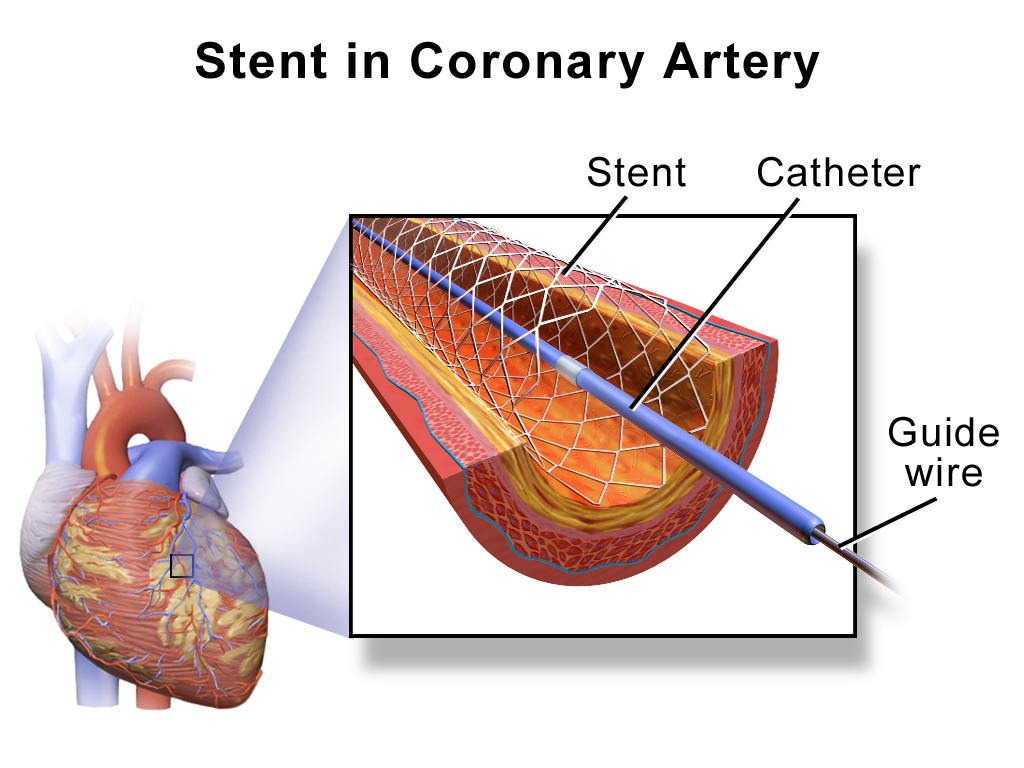
Researchers from Stanford University School of Medicine believe they’ve found a drug for cardiac stents that can more effectively prevent stent complications.
Over a million people in the U.S. each year undergo angioplasty heart surgery using a drug-coated stent to treat blocked arteries, according to the American Heart Association. A stent is a tiny wire mesh tube that is permanently implanted into the artery at the blockage point, creating a scaffold that props open the artery to reduce the chance of a heart attack. However, placement of bare metal stents can themselves damage the artery lining, causing scar tissue to grow and narrow the artery. Known as in-stent stenosis, this typically occurs 3-6 months after the surgical procedure and can lead to chest pain and even heart attacks.
To help prevent in-stent stenosis, doctors use stents coated with drugs that inhibit tissue regrowth to help prevent the blood vessels from reclosing. Unfortunately, these drugs can also inhibit beneficial regrowth of the vessel’s blood lining (endothelium) that aids the healing process. So patients still need to take blood-thinners for up to a year to reduce the risk of a blood clot developing in the stent and blocking the artery. This need for blood thinners is a serious problem for many people with other health issues; for instance, it means they can’t have surgery while taking the medication.
Stanford researchers have now identified a drug to coat cardiac stents that helps prevent in-stent stenosis without affecting the healing of the blood vessel lining. Their new research is described in a paper published this month in the Journal of Clinical Investigation. Dr. Euan Ashley, associate professor of cardiovascular medicine and genetics at Stanford University Medical Center, led the research team.
The researchers first sought to more fully understand the genetic pathways of coronary artery disease using a “big data” computational biology approach. Using data from previous studies, they analyzed large datasets of coronary artery tissue samples and genome information from patients who had developed in-stent stenosis after undergoing angioplasty and stenting. Based on network analyses, the researchers hypothesized that there is an increased risk of in-stent stenosis due to the interplay of two genes, GPX1 and ROS1.
GPX1 deficiency is known to be independently associated with coronary artery disease in humans. However, ROS1 expression is mostly known for its role in highly malignant cancers, such as lung cancers.
“We didn’t know anything about ROS1,” said Ashley in a press release. “It hadn’t been studied in cardiovascular disease. We knew it was an important gene in cancer. We thought, that’s odd, since the growth caused by stents is almost like a tumor.”
They confirmed their theory by performing an extensive series of laboratory experiments using human tissue samples and genetically engineered knockout mice. Some of these studies involved surgically implanting drug-coated stents in mice with clogged arteries. The researchers inhibited the ROS1 genes by coating these stents with crizotinib – a chemotherapy drug used to treat certain ROS1-positive lung cancers. They found that crizotinib inhibited in-stent stenosis without affecting the lining of the blood vessels.
“The major finding of the study is that artery stent disease acts surprisingly like a tumor in the blood vessel wall,” said Ashley in the press release. “Inhibiting it with nonspecific pharmaceutical agents, as we do now, leads to heart attacks from clots caused by lack of endothelial lining on the stent. Whereas, targeting it with the drug we use here, crizotinib, acts much more specifically and inhibits the disease without affecting the endothelium.”
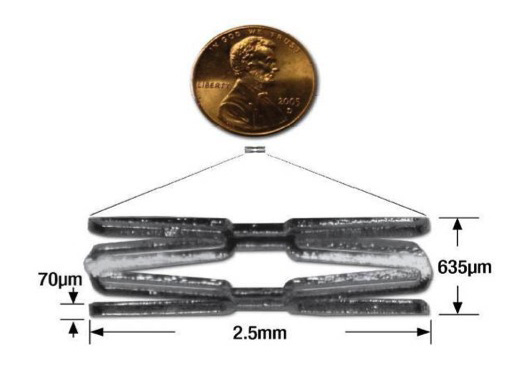
A tiny mouse-sized stent used by Stanford researchers in their mice studies. (Courtesy of Euan Ashley)
Stanford researchers still have a lot more work to do before crizotinib-coated stents will be clinically available. However, this research should translate to the clinic more quickly since crizotinib is already an FDA approved drug.
LBNL Institute for Globally Transformative Technologies research team with prototype vaccine fridge and backpack for developing countries. (Berkeley Lab / Roy Kaltschmidt)
Vaccines are arguably one of the most important inventions of mankind. Unfortunately, vaccines must be produced and stored in an environment with very tight temperature regulation – between 36 °F and 46 °F – to keep the vaccine bugs alive. So vaccine delivery is a major problem due to the absence of reliable refrigeration in many remote countries.
Approximately 30 million children worldwide – roughly one in five – do not receive immunizations, leaving them at significant risk of disease. As a result, 1.5 million children under the age of five die annually from vaccine-preventable diseases, such as pneumonia and diarrhea. Perhaps more surprising, almost half of the vaccines in developing countries are thrown away because they get too warm during delivery so they are no longer viable. Some administered vaccines are also ineffective because they froze during transport, but there is no easy way to test this.
Scientists at Lawrence Berkeley National Laboratory (LBNL) are trying to solve this vaccine delivery problem by developing a portable solar-powered fridge. Fabricated entirely at LBNL, their portable solar-powered vaccine fridge will be transported by bicycle or motorcycle in remote areas of the developing world. Zach Friedman and Reshma Singh are leading the project as part of the LBNL Institute for Globally Transformative Technologies, which seeks to bring scientific and technological breakthroughs to address global poverty and related social ills.
The team’s first prototype portable fridge uses a thermoelectric heat pump, rather than a traditional vapor compression heat pump that relies on a circulating liquid refrigerant to absorb and remove heat. The thermoelectric chips were initially developed to keep laptops cool, so laptops could be made thinner without fans. The technology was adapted for this global application to reduce the size and weight of the fridge.
Their portable units have a one to three-liter capacity, much smaller than standard solar fridges that are typically 50 liters or more. Once the fridge cools down to the right temperature (36 °F – 46 °F), it is designed to run within that temperature range for at least five days without any power, at an ambient outside temperature as hot as 110 °F.
Before the researchers can field test their first prototype fridge in Africa, they need to pass the World Health Organization’s Performance, Quality and Safety testing protocol for products used in immunization programs. They are currently busy performing in-house testing at LBNL to ensure that they pass the formal tests, which will be conducted by an independent laboratory in the UK.
“We aren’t in the process of field testing yet, but we have established field testing agreements in both Kenya and Nigeria and have locations identified,” said Friedman. “We expect to start testing this coming year.”
Meanwhile, they are continuing their portable fridge development. “Currently, we are pursuing both thermoelectric and vapor compression heat pumps, even for these smaller devices,” explained Jonathan Slack, lead engineer. “It is not clear which will win out in terms of manufacturability and affordability.”
They are also developing a backpack version of the vaccine fridge. However, human-carried devices have to meet stricter World Health Organization standards, so they are focusing at this stage on the small portable fridge instead.
Ultimately their goal is to make it easy for health care workers to deliver viable vaccines to children in remote areas, solving the “last miles” of vaccine delivery.
Kindergartener learning to read a book (Holtsman/flickr)
For many, the word dyslexia represents painful struggles with reading and speech that impact their self-confidence –- 20 percent of school-aged children and over 40 million adults in the U.S. are dyslexic. Dyslexics are often very intelligent and can learn successfully with appropriate teaching methods, but early diagnosis and intervention are critical.
UC San Francisco (UCSF) researchers in the Dyslexia Program aim to predict whether children will develop dyslexia before they show signs of reading and speech problems, so early intervention can improve their quality of life.
“Early identification and interventions are extremely important in children with dyslexia as well as most neurodevelopmental disorders,” said Fumiko Hoeft, UCSF associate professor and member of the UCSF Dyslexia Center, in a press release. “Accumulation of research data such as ours may one day help us to identify kids who might be at risk for dyslexia, rather than waiting for children to become poor readers and experience failure.”
In a recent longitudinal study, Hoeft’s research team studied 38 young children using structural MRI to track their brain development between kindergarten and third grade as they formally learned to read in school. The participating children were healthy, native-English speakers with varying preliteracy skills and family histories of reading difficulties. They had MRI brain scans at age 5 or 6 and again 3 years later. At both time points, they also completed a battery of standardized tests, including reading and cognitive assessments.
In particular, the researchers were interested in the children’s white matter development, which is critical for perceiving, thinking and learning. They found that volume changes in the left hemisphere white matter in the temporo-parietal region (just behind and above the left ear) was highly predictive of reading outcomes. This region is known to be important for language, reading and speech.
Using MRI brain scans to measure these developmental changes improved the prediction accuracy of reading difficulties by 60%, compared to traditional assessments alone.
“What was intriguing in this study was that brain development in regions important to reading predicted above and beyond all these (other) measures,” said Hoelt.
Despite this predictive relationship, MRI brain imaging is unlikely to be a widespread means of diagnosis because of cost and time constraints. Instead, the researchers hope their findings lead to further investigation of what may be influencing the brain during this critical period of reading development.
The UCSF Dyslexia Center is also investigating cheaper methods for early diagnosis of reading problems. For example, they are collaborating with research labs worldwide to construct growth charts for the reading brain network, similar to those one would find in a doctor’s office for height and weight.
Since screening for reading disorder risk is currently a resource-intensive process, UCSF is also developing a tablet-based mobile health application that could be used by schools or parents as a fast, easy and cheap screening tool.
UCSF researchers hope that understanding each child’s neurocognitive profile will help educators provide improved, personalized education and interventions.
Eyeglasses may no longer be necessary to see computer screens. (F H Mira, flickr)
What if everyone could clearly see their smart phone, tablet, computer and TV screens without having to wear corrective eyeglasses or contact lenses?
Approximately 75% of American adults use some form of corrective lenses to see or read properly. And most of us need them to see computer screens on a daily basis. Now researchers are developing new technology that uses computer algorithms to compensate for an individual’s visual impairment, so many of us may soon be able to ditch our glasses and contacts.
Brian Barsky, UC Berkeley professor of computer science and vision science and affiliate professor of optometry, teamed up with colleagues at UC Berkeley and MIT to improve vision-correcting display technology. They developed a combination of hardware and software improvements to achieve both high image resolution and contrast simultaneously, a major milestone. Their results were recently published in a paper in the ACM Transactions on Graphics.
First, they modified an iPod touchscreen by adding a standard light field display – a mask with an array of pinholes sandwiched between thin layers of plastic. The tiny pinholes were each 75 micrometers in diameter and spaced 390 micrometers apart. This light field display was used to enhance image contrast, providing a full range of bright colors in the displayed images.
The researchers also developed complex, innovative computer algorithms to adjust the light intensity from each pinhole. These algorithms helped enhance the resolution or sharpness of the displayed images. The researchers can use a person’s eyeglass prescription to compute an altered image, that when viewed through the light field display, appears in sharp focus for that individual.
“Our technique distorts the image such that, when the intended user looks at the screen, the image will appear sharp to that particular viewer,” said Barsky in a press release. “But if someone else were to look at the image, it would look bad.”
The technology could not only help the millions of people who wear glasses and contacts, but also those with complex vision problems that cannot be corrected. The most common vision problems – nearsightedness, farsightedness and astigmatism – are usually easily corrected with standard lenses. However, people with complex vision problems often have irregularities in the shape of their eyes’ surface or cornea, requiring new kinds of corrective lenses that are still under development.
“We now live in a world where displays are ubiquitous, and being able to interact with displays is taken for granted,” said Barsky. “People who are unable to view displays are at a disadvantage in the workplace and life in general, so this research could transform their lives.”
In the future, the researchers plan to incorporate commercially available eye trackers to adapt the displayed images to the user’s head position. They also hope to develop display screens that appear clear to multiple users with different visual problems.
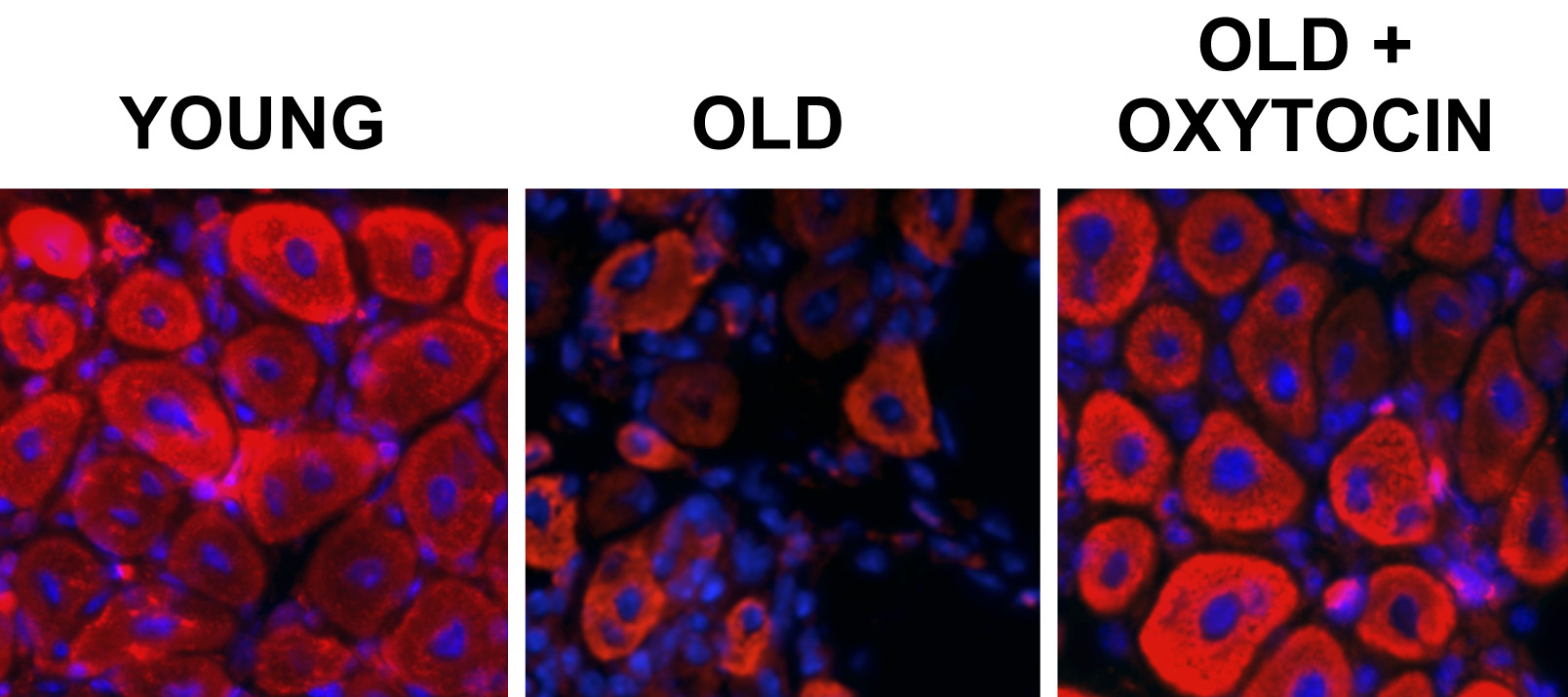
The left image shows healthy muscle tissue from a young mouse. The middle image demonstrates that the efficiency of muscle repair mechanisms decreases with age, resulting in a lower density of muscle fibers and increased scar tissue in an old mouse. Injecting oxytocin rapidly rejuvenates the old tissue, as shown on the right image. (Wendy Cousin and Christian Elabd)
From birth until about the age of 30, your muscles continue to grow larger and stronger. But at some point in your 30s, you begin to lose muscle mass and strength which in turn affects your coordination. As part of the natural aging process, this disease, sarcopenia, is most commonly seen in inactive people but it also affects those who remain physically active throughout their lives.
Now UC Berkeley researchers have discovered that oxytocin – the “trust hormone” associated with maternal nurturing, social attachments, childbirth and sex – may combat this age-related muscle wasting. Their new study was recently published in Nature Communications.
Role in Muscle Regeneration
Led by associate professor of bioengineering Irina Conboy, the researchers found in mice that oxytocin is required to maintain healthy muscles, but the level of oxytocin in the blood and the number of oxytocin receptors in muscle stem cells naturally reduce with age. For instance, old (18 to 24 months) mice were found to have 3 times lower circulating levels of oxytocin than young (2 to 4 months) mice.
The research team performed a series of experiments using young and old mice to better understand oxytocin’s role in muscle repair. They injected the mice daily with oxytocin (or a control solution) under the skin for nine consecutive days, while causing a muscle injury midway on day 4. The researchers found that the old mice that received the oxytocin were able to repair their muscle injury at a level comparable to the young mice – far better than the old control group that didn’t get oxytocin. Systemic administration of oxytocin appears to rapidly improve muscle regeneration by enhancing aged muscle stem cell proliferation.
In contrast, the young mice already had sufficient levels of oxytocin and efficient muscle regeneration, so the oxytocin injections had no significant effect. This is important since most molecules that boost tissue repair are also associated with an increased risk of cancer.
“This is good because it demonstrates that extra oxytocin boosts aged tissue stem cells without making muscle stem cells divide uncontrollably,” explained Wendy Cousin, a senior scientist in Conboy’s lab, in a press release.
The researchers also performed similar experiments using mice with an inactivated gene for oxytocin and control mice. At the young age of 3 months, the two groups of mice appeared to have comparable muscle mass and repair efficiency after a muscle injury. However, muscle atrophy and a significant decline in muscle regeneration were observed for the 1-year old adult mice with the disabled oxytocin gene, signifying premature aging due to a lack of oxytocin.
It is unclear how long it will take the researcher to move beyond mice studies to human use. However, oxytocin is already approved by the FDA for clinical use in humans for other applications. For instance, oxytocin is commonly used to help increase contractions and control bleeding during childbirth. So getting approval for human studies should be straightforward once the researchers are ready.
Conboy’s research team is ultimately interested in applications beyond just maintaining healthy muscles. For instance, they are also investigating whether oxytocin could become a viable alternative to hormone replacement therapy to impede the symptoms of male and female aging. They also believe that aging is the underlying cause of a number of chronic diseases, including Parkinson’s and Type 2 diabetes.
Oxytocin Hype
In fact, researchers around the world are studying the use of oxytocin for seemingly every condition imaginable, including using oxytocin nasal spray to alleviate symptoms associated with mental disorders such as autism, schizophrenia and dementia. However, this research currently demonstrates mixed and inconsistent results, particularly regarding oxytocin’s influence on social skills.
The current excitement about oxytocin, particularly as a remedy for autism, could lead to a dangerous situation given the widespread availability of oxytocin supplements – as an accelerator spray, sublingual liquid that is absorbed under the tongue, pills and mouth lozenges. It is important to consult with your doctor before taking oxytocin.